Acute respiratory infections are a major cause of morbidity and hospitalisation in children. In this context, respiratory multiplex Polymerase chain reaction (PCR) is a rapid molecular tool enabling the simultaneous identification of several pathogens. The objective of this study was to evaluate the diagnostic contribution of multiplex PCR in paediatric respiratory infections, to describe the epidemiological profile of the patients managed, and to analyse the concordance between PCR results and certain commonly used biological markers, notably C-reactive protein (CRP) and white blood cell count. This was a retrospective descriptive study conducted at the Mohammed V Military Teaching Hospital in Rabat. It included 125 children under the age of 5, hospitalised between September 2021 and September 2025. Respiratory samples were analysed using the FilmArray Respiratory Panel, enabling the simultaneous detection of 16 viruses and 4 bacteria. Clinical and laboratory data were extracted from the DX Lab software. Of the 125 samples analysed, 90 were positive, representing a positivity rate of 72%. In total, 122 pathogens were identified. Viral infections were overwhelmingly predominant, dominated by Rhinovirus/Enterovirus, followed by respiratory syncytial virus (RSV) and severe acute respiratory syndrome Coronavirus 2 (SARS-CoV-2). Bacterial detections were rare. Co-infections were present in more than a third of the positive samples, primarily in the form of viral combinations. Biologically, nearly half of patients with a positive PCR result had normal CRP levels, while the majority had a white blood cell count appropriate for their age, with no systematic correlation with PCR positivity. Respiratory multiplex PCR thus appears to be a highly effective diagnostic tool in the management of paediatric respiratory infections. It enables rapid and reliable identification of infectious agents, improves therapeutic management and may help to limit the inappropriate use of antibiotics. These results support its value in the hospital management of respiratory infections in children in Morocco.
| Published in | American Journal of Pediatrics (Volume 12, Issue 2) |
| DOI | 10.11648/j.ajp.20261202.14 |
| Page(s) | 76-86 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Respiratory Multiplex PCR, Acute Respiratory Infections, Paediatrics, FilmArray, Molecular Diagnostics, Morocco
Viruses | Viruses (cont.) | Bacteria |
|---|---|---|
Coronavirus HKU1 | Influenza A virus | Mycoplasma pneumoniae |
Coronavirus NL63 | Influenza B virus | Bordetella parapertussis |
Coronavirus 229E | Parainfluenza virus 1 | Chlamydophila pneumoniae |
Coronavirus OC43 | Parainfluenza virus 2 | Mycoplasma pneumoniae |
Human Metapneumovirus | Parainfluenza virus 3 | |
Human Rhinovirus/Enterovirus | Parainfluenza virus 4 | |
SARS-CoV-2 | Respiratory Syncytial Virus (RSV) | |
MERS-CoV | Adenovirus |
Age group | Number | Percentage |
|---|---|---|
< 1 year | 6 | 4.8% |
1–2 years | 29 | 23.2% |
3–4 years | 80 | 64.0% |
5 years | 10 | 8.0% |
Total | 125 | 100% |
Year | Number | Percentage |
|---|---|---|
2021/2022 | 18 | 14.4% |
2022/2023 | 77 | 61.6% |
2023/2024 | 9 | 7.2% |
2024/2025 | 21 | 16.8% |
Total | 125 | 100% |
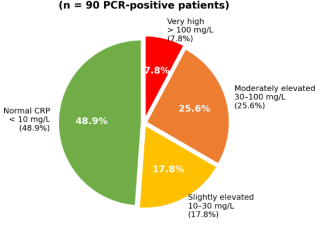
CRP | Number | Percentage |
|---|---|---|
Normal (< 10 mg/L) | 59 | 47.2% |
Slightly elevated (10–30 mg/L) | 24 | 19.2% |
Moderately elevated (30–100 mg/L) | 29 | 23.2% |
Very high (> 100 mg/L) | 13 | 10.4% |
Total | 125 | 100% |
White blood cells | Number | Percentage |
|---|---|---|
Normal values | 85 | 68.0% |
Moderate leukocytosis | 37 | 29.6% |
Marked leukocytosis | 3 | 2.4% |
Total | 125 | 100% |
PCR result | Number | Percentage |
|---|---|---|
Positive | 90 | 72.0% |
Negative | 32 | 25.6% |
Not performed | 3 | 2.4% |
Total | 125 | 100% |
Category | Number of detections | Number of species |
|---|---|---|
Viruses | 118 | 13 |
Bacteria | 4 | 3 |
Total | 122 | 16 |
Virus | Number | Percentage |
|---|---|---|
Rhinovirus/Enterovirus | 50 | 42.4% |
RSV | 18 | 15.3% |
SARS-CoV-2 | 14 | 11.9% |
Adenovirus | 12 | 10.2% |
Parainfluenza 3 | 7 | 5.9% |
Metapneumovirus | 5 | 4.2% |
Seasonal coronaviruses | 4 | 3.4% |
Influenza B | 3 | 2.5% |
Parainfluenza 2 | 3 | 2.5% |
Influenza A | 2 | 1.7% |
Total | 118 | 100% |
Bacterium | Number |
|---|---|
Bordetella pertussis | 2 |
Mycoplasma pneumoniae | 1 |
Chlamydophila pneumoniae | 1 |
Total | 4 |
Type of infection | Number | Percentage |
|---|---|---|
Mono-infection | 58 | 64.4% |
Virus–virus co-infection | 28 | 31.1% |
Virus–bacterium co-infection | 4 | 4.5% |
Total | 90 |
Pathogen | Agent type | Mono-infections | Co-infections | Total detections |
|---|---|---|---|---|
Rhinovirus/Enterovirus | Virus | 27 | 23 | 50 |
RSV | Virus | 9 | 9 | 18 |
SARS-CoV-2 (COVID-19) | Virus | 7 | 7 | 14 |
Adenovirus | Virus | 3 | 9 | 12 |
Parainfluenza 3 | Virus | 3 | 4 | 7 |
Metapneumovirus | Virus | 2 | 3 | 5 |
Coronavirus OC43 | Virus | 1 | 1 | 2 |
Coronavirus NL63 | Virus | 1 | 1 | 2 |
Coronavirus NL63 | Virus | 0 | 1 | 1 |
Coronavirus 229E | Virus | 0 | 1 | 1 |
Parainfluenza 2 | Virus | 1 | 2 | 3 |
Influenza B | Virus | 2 | 1 | 3 |
Influenza A | Virus | 2 | 0 | 2 |
Bordetella pertussis | Bacterium | 0 | 2 | 2 |
Chlamydophila pneumoniae | Bacterium | 0 | 1 | 1 |
Mycoplasma pneumoniae | Bacterium | 0 | 1 | 1 |
Total | – | 58 | 64 | 122 |
Country | Predominant age group | Reference |
|---|---|---|
Our study | 3–4 years | – |
United States | < 5 years (median ≈ 2 years) | 53 |
Netherlands | 1–5 years | 51 |
Spain | 1–5 years | 52 |
Morocco | 6–23 months | 54 |
Morocco/North Africa | < 2 years | 55 |
Study/Country | Sex ratio | Reference |
|---|---|---|
Our study | 1.36 | – |
Malaysia | 1.4 | 56 |
Italy | 1.3 | 57 |
China | 1.2–1.5 | 58, 59 |
France | 1.2 | 60 |
Morocco | > 1 | 61 |
Cambodia | 0.8 | 62 |
Study | Total sample size | Number positive | Positivity rate (%) |
|---|---|---|---|
Our study | 125 | 90 | 72% |
Egypt | 177 | 166 | 93.8% |
Italy | 356 | 302 | 84.7% |
Belgium | 149 | 125 | 83.9% |
China | 775 | 626 | 80.8% |
Turkey | 536 | 258 | 48.2% |
United States | 438 | 201 | 45.9% |
Study | Most frequent virus | Frequency (%) |
|---|---|---|
Our study | Rhinovirus/Enterovirus | 42.40 |
France | RSV | 39.50 |
China | Rhinovirus/Enterovirus | 25.50 |
Ghana | Rhinovirus/Enterovirus | 36.00 |
Central African Republic | Rhinovirus/Enterovirus | 40.00 |
HMIMV | Mohammed V Military Teaching Hospital |
PCR | Polymerase Chain Reaction |
CRP | C-reactive Protein |
ARIs | Acute Respiratory Infections |
RSV | Respiratory Syncytial Virus |
SARS | Cov 2 Severe Acute Respiratory Syndrome Coronavirus 2 |
MERS | Cov Middle East Respiratory Syndrome Coronavirus |
| [1] | Williams BG, Gouws E, Boschi-Pinto C, Bryce J, Dye C. Estimates of world-wide distribution of child deaths from acute respiratory infections. Lancet Infect Dis. 2002; 2(1): 25-32. |
| [2] | McIntosh K. Community-acquired pneumonia in children. N Engl J Med. 2002; 346(6): 429-437. |
| [3] | Ministry of Health, Morocco. Health in Figures 2022. |
| [4] | Poritz MA, et al. FilmArray, an Automated Nested Multiplex PCR System for Multi-Pathogen Detection. PLoS ONE. 2011; 6(10): e26047. |
| [5] | Chen YS, et al. Comparison of diagnostic tools with multiplex PCR for pediatric lower respiratory tract infection. J Microbiol Immunol Infect. 2013; 46(6): 413-8. |
| [6] | BioFire FilmArray Respiratory Panel. bioMérieux. |
| [7] | Monto AS. Viral respiratory infections in the community. Am J Med. 1995; 99(6B): 24S-27S. |
| [8] | Wishaupt JO, et al. Single- and multiple viral respiratory infections in children. BMC Infect Dis. 2017; 17(1): 62. |
| [9] | Mengelle C, et al. Multiplex real-time PCR for diagnosing acute respiratory viral infections in children. J Clin Virol. 2014; 61(3): 411-7. |
| [10] | Jain S, et al. Community-acquired pneumonia requiring hospitalization among U.S. children. N Engl J Med. 2015; 372(9): 835-45. |
| [11] | Evolution of acute lower respiratory infections in children under 5 in Morocco. EM-Consulte. |
| [12] | Jroundi I, et al. Knowledge gaps on paediatric respiratory infections in Morocco. Arch Public Health. 2015; 73(1): 28. |
| [13] | Khor CS, et al. Epidemiology and seasonality of respiratory viral infections in Kuala Lumpur. BMC Pediatr. 2012; 12: 32. |
| [14] | Ciotti M, et al. Viruses of Respiratory Tract: An Observational Retrospective Study in Rome. Microorganisms. 2020; 8(4): 501. |
| [15] | Li J, et al. Rapid detection of respiratory organisms with FilmArray in China. BMC Infect Dis. 2018; 18(1): 510. |
| [16] | Deng J, et al. Respiratory virus multiplex RT-PCR assay sensitivities in hospitalized children. Virol Sin. 2013; 28(2): 97-102. |
| [17] | Koenig-Zores C, et al. Virological analysis of nasopharyngeal aspirates in children by multiplex PCR. Rev Fr Allergol. 2013; 53(2): 59-64. |
| [18] | Lamrani Hanchi A, et al. Epidemiology of Respiratory Pathogens in Children with SARI. Int J Microbiol. 2021; 2021: 2276261. |
| [19] | Ly N, et al. Multiplex PCR analysis of clusters of unexplained viral respiratory tract infection in Cambodia. Virol J. 2014; 11(1): 224. |
| [20] | Zanotto E, et al. Impact of COVID-19 Pandemic on Respiratory Pathogen Epidemiology. Sci. 2025; 7(1): 23. |
| [21] | Korppi M, Kröger L. C-reactive protein in viral and bacterial respiratory infection in children. Scand J Infect Dis. 1993; 25(2): 207-13. |
| [22] | Babu G, et al. Value of CRP concentration in diagnosis of acute lower respiratory infections. Trop Geogr Med. 1989; 41(4): 309-15. |
| [23] | De Rop L, et al. Point-of-care CRP test results in acute infections in children. BMC Pediatr. 2022; 22(1): 633. |
| [24] | Adar A, et al. CRP Is Associated with Severity in RSV Bronchiolitis. Isr Med Assoc J. 2025; 27(3): 165-71. |
| [25] | MSD Manuals. Lymphopenia – Blood Disorders. |
| [26] | Gad NM, et al. Viral Infections in Egyptian Hospitalized Children with ARI. J Clin Cell Immunol. 2017; 8(5). |
| [27] | Ye X, et al. Bacterial Pneumonia Alters the Respiratory Microbiota. Curr Microbiol. 2025; 82(11): 528. |
| [28] | Cebey-López M, et al. Viral Co-Infections in Pediatric Patients with Lower Tract ARI. PLoS One. 2015; 10(9): e0136526. |
| [29] | del Rosal T, et al. Multiplex PCR and Antibiotic Use in Children with Community-Acquired Pneumonia. Children. 2024; 11(2): 245. |
| [30] | Busson L, et al. Contribution of FilmArray in emergency room management during influenza epidemics. Int J Infect Dis. 2019; 83: 32-9. |
| [31] | The use of multiplex PCR for the diagnosis of viral SARI in children. ResearchGate. |
| [32] | Keske Ş, et al. Rapid diagnosis of viral respiratory tract infections and antimicrobial stewardship. Eur J Clin Microbiol Infect Dis. 2018; 37(4): 779-83. |
| [33] | Katz SE, Williams DJ. Pediatric Community-Acquired Pneumonia in the United States. Infect Dis Clin North Am. 2018; 32(1): 47-63. |
| [34] | Gowin E, et al. Assessment of Multiplex Real-Time PCR Tests in Pneumonia in Hospitalized Children. Biomed Res Int. 2017; 2017: 8037963. |
| [35] | Wilson PT, et al. Respiratory Pathogens in Children in Ghana. J Pediatric Infect Dis Soc. 2019; 8(4): 361-4. |
| [36] | Bobossi Serengbe G, et al. Viral aetiology of acute respiratory infections in children in Bangui. Arch Pediatr. 2015; 22(3): 324-5. |
| [37] | Dierig A, et al. Mycoplasma pneumoniae detection in children in Switzerland. Acta Paediatrica. 2020; 109(2): 375-80. |
| [38] | Merida Vieyra J, et al. Chlamydophila pneumoniae-associated community-acquired pneumonia in paediatric patients in Mexico. Sci Rep. 2023; 13(1): 21477. |
| [39] | Seasonality and prevalence of respiratory pathogens detected by multiplex PCR at a tertiary care medical center. PubMed. |
| [40] | Multiple versus single virus respiratory infections: viral load and clinical disease severity in hospitalized children. PubMed. |
| [41] | Mahony JB. Detection of respiratory viruses by molecular methods. Clin Microbiol Rev. 2008; 21(4): 716-47. |
APA Style
Ouhrich, I., Abi, R., Akhssas, A., Laasikri, I., Bennamara, F. Z., et al. (2026). The Role of Respiratory Multiplex PCR in Acute Respiratory Infections in Children Under 5 Years of Age: Experience of the Mohammed V Military Teaching Hospital in Rabat. American Journal of Pediatrics, 12(2), 76-86. https://doi.org/10.11648/j.ajp.20261202.14
ACS Style
Ouhrich, I.; Abi, R.; Akhssas, A.; Laasikri, I.; Bennamara, F. Z., et al. The Role of Respiratory Multiplex PCR in Acute Respiratory Infections in Children Under 5 Years of Age: Experience of the Mohammed V Military Teaching Hospital in Rabat. Am. J. Pediatr. 2026, 12(2), 76-86. doi: 10.11648/j.ajp.20261202.14
AMA Style
Ouhrich I, Abi R, Akhssas A, Laasikri I, Bennamara FZ, et al. The Role of Respiratory Multiplex PCR in Acute Respiratory Infections in Children Under 5 Years of Age: Experience of the Mohammed V Military Teaching Hospital in Rabat. Am J Pediatr. 2026;12(2):76-86. doi: 10.11648/j.ajp.20261202.14
@article{10.11648/j.ajp.20261202.14,
author = {Issam Ouhrich and Rachid Abi and Anouar Akhssas and Imane Laasikri and Fatima Zahra Bennamara and Abir Belahrach and Manal Najib and Hind Azzouzi and Nada Mchichou and Zahira Bouassaba and Elarbi Bouaiti and Mohamed-Rida Tagajdid and Hicham Elannaz and Salma Hassine and Soukaina Ouannass and Ahmad Reggad and Mohamed Elqatni and Abdelilah Laraqui and Abdelilah Radi and Hakim Ourrai and Rachid Abilkassem and Mostafa Elouennass and Khalid Ennibi and Idriss Lahlou Amine},
title = {The Role of Respiratory Multiplex PCR in Acute Respiratory Infections in Children Under 5 Years of Age: Experience of the Mohammed V Military Teaching Hospital in Rabat},
journal = {American Journal of Pediatrics},
volume = {12},
number = {2},
pages = {76-86},
doi = {10.11648/j.ajp.20261202.14},
url = {https://doi.org/10.11648/j.ajp.20261202.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20261202.14},
abstract = {Acute respiratory infections are a major cause of morbidity and hospitalisation in children. In this context, respiratory multiplex Polymerase chain reaction (PCR) is a rapid molecular tool enabling the simultaneous identification of several pathogens. The objective of this study was to evaluate the diagnostic contribution of multiplex PCR in paediatric respiratory infections, to describe the epidemiological profile of the patients managed, and to analyse the concordance between PCR results and certain commonly used biological markers, notably C-reactive protein (CRP) and white blood cell count. This was a retrospective descriptive study conducted at the Mohammed V Military Teaching Hospital in Rabat. It included 125 children under the age of 5, hospitalised between September 2021 and September 2025. Respiratory samples were analysed using the FilmArray Respiratory Panel, enabling the simultaneous detection of 16 viruses and 4 bacteria. Clinical and laboratory data were extracted from the DX Lab software. Of the 125 samples analysed, 90 were positive, representing a positivity rate of 72%. In total, 122 pathogens were identified. Viral infections were overwhelmingly predominant, dominated by Rhinovirus/Enterovirus, followed by respiratory syncytial virus (RSV) and severe acute respiratory syndrome Coronavirus 2 (SARS-CoV-2). Bacterial detections were rare. Co-infections were present in more than a third of the positive samples, primarily in the form of viral combinations. Biologically, nearly half of patients with a positive PCR result had normal CRP levels, while the majority had a white blood cell count appropriate for their age, with no systematic correlation with PCR positivity. Respiratory multiplex PCR thus appears to be a highly effective diagnostic tool in the management of paediatric respiratory infections. It enables rapid and reliable identification of infectious agents, improves therapeutic management and may help to limit the inappropriate use of antibiotics. These results support its value in the hospital management of respiratory infections in children in Morocco.},
year = {2026}
}
TY - JOUR T1 - The Role of Respiratory Multiplex PCR in Acute Respiratory Infections in Children Under 5 Years of Age: Experience of the Mohammed V Military Teaching Hospital in Rabat AU - Issam Ouhrich AU - Rachid Abi AU - Anouar Akhssas AU - Imane Laasikri AU - Fatima Zahra Bennamara AU - Abir Belahrach AU - Manal Najib AU - Hind Azzouzi AU - Nada Mchichou AU - Zahira Bouassaba AU - Elarbi Bouaiti AU - Mohamed-Rida Tagajdid AU - Hicham Elannaz AU - Salma Hassine AU - Soukaina Ouannass AU - Ahmad Reggad AU - Mohamed Elqatni AU - Abdelilah Laraqui AU - Abdelilah Radi AU - Hakim Ourrai AU - Rachid Abilkassem AU - Mostafa Elouennass AU - Khalid Ennibi AU - Idriss Lahlou Amine Y1 - 2026/06/12 PY - 2026 N1 - https://doi.org/10.11648/j.ajp.20261202.14 DO - 10.11648/j.ajp.20261202.14 T2 - American Journal of Pediatrics JF - American Journal of Pediatrics JO - American Journal of Pediatrics SP - 76 EP - 86 PB - Science Publishing Group SN - 2472-0909 UR - https://doi.org/10.11648/j.ajp.20261202.14 AB - Acute respiratory infections are a major cause of morbidity and hospitalisation in children. In this context, respiratory multiplex Polymerase chain reaction (PCR) is a rapid molecular tool enabling the simultaneous identification of several pathogens. The objective of this study was to evaluate the diagnostic contribution of multiplex PCR in paediatric respiratory infections, to describe the epidemiological profile of the patients managed, and to analyse the concordance between PCR results and certain commonly used biological markers, notably C-reactive protein (CRP) and white blood cell count. This was a retrospective descriptive study conducted at the Mohammed V Military Teaching Hospital in Rabat. It included 125 children under the age of 5, hospitalised between September 2021 and September 2025. Respiratory samples were analysed using the FilmArray Respiratory Panel, enabling the simultaneous detection of 16 viruses and 4 bacteria. Clinical and laboratory data were extracted from the DX Lab software. Of the 125 samples analysed, 90 were positive, representing a positivity rate of 72%. In total, 122 pathogens were identified. Viral infections were overwhelmingly predominant, dominated by Rhinovirus/Enterovirus, followed by respiratory syncytial virus (RSV) and severe acute respiratory syndrome Coronavirus 2 (SARS-CoV-2). Bacterial detections were rare. Co-infections were present in more than a third of the positive samples, primarily in the form of viral combinations. Biologically, nearly half of patients with a positive PCR result had normal CRP levels, while the majority had a white blood cell count appropriate for their age, with no systematic correlation with PCR positivity. Respiratory multiplex PCR thus appears to be a highly effective diagnostic tool in the management of paediatric respiratory infections. It enables rapid and reliable identification of infectious agents, improves therapeutic management and may help to limit the inappropriate use of antibiotics. These results support its value in the hospital management of respiratory infections in children in Morocco. VL - 12 IS - 2 ER -
Laboratory Department, Mohammed V University, Rabat, Morocco
Centre of Virology Infectious and Tropical Diseases (CVMIT), Mohamed V Military Teaching Hospital, Rabat, Morocco
Information